Drunk User Interfaces: Determining Blood Alcohol Level
through Everyday Smartphone Tasks
Alex Mariakakis
1
, Sayna Parsi
2,3
, Shwetak N. Patel
1
, Jacob O. Wobbrock
3
1
Computer Science & Engineering,
2
Human Centered Design & Engineering,
3
The Information School
DUB Group
University of Washington
Seattle, WA 98195 USA
{atm15, shwetak}@cs.washington.edu, {parsis, wobbrock}@uw.edu
ABSTRACT
Breathalyzers, the standard quantitative method for
assessing inebriation, are primarily owned by law
enforcement and used only after a potentially inebriated
individual is caught driving. However, not everyone has
access to such specialized hardware. We present drunk user
interfaces: smartphone user interfaces that measure how
alcohol affects a person’s motor coordination and cognition
using performance metrics and sensor data. We examine
five drunk user interfaces and combine them to form the
“DUI app”. DUI uses machine learning models trained on
human performance metrics and sensor data to estimate a
person’s blood alcohol level (BAL). We evaluated DUI on
14 individuals in a week-long longitudinal study wherein
each participant used DUI at various BALs. We found that
with a global model that accounts for user-specific learning,
DUI can estimate a person’s BAL with an absolute mean
error of 0.005% ± 0.007% and a Pearson’s correlation
coefficient of 0.96 with breathalyzer measurements.
Author Keywords
Situational impairments; alcohol; mobile; smartphones;
health; drunkenness; inebriation; safety; driving.
ACM Classification Keywords
K.4.1. Computers and Society: Public Policy Issues –
human safety; J.3. Computer applications: Life and Medical
Sciences – health.
INTRODUCTION
In 2014, 27 people died every day as a result of drunk
driving in the United States [35]. Portable breathalyzers
were invented in 1931 [19] to allow law enforcement to
prosecute cases of drunk driving; however, breathalyzers
are typically used after a drunk driver has been caught,
rarely to prevent people from driving in the first place.
Jewett et al. [14,23] estimate that the average drunk driver
has driven drunk over 80 times before their first arrest.
There remains a need of being able to catch cases of drunk
driving without the presence of law enforcement or relying
on people to determine their own limits for personal safety.
One can view inebriation as a temporary “situational
impairment” that affects a person as they interact with the
world around them [36,40,41,46,51]. From this ability-
based perspective, we propose drunk user interfaces
(DUIs): smartphone-based tasks that challenge and assess a
person’s motor coordination and cognition. When a person
manipulates a drunk user interface, the smartphone can
measure how well that person performs the required task
using human performance metrics and features derived
from embedded sensors (e.g., the touchscreen,
accelerometer). For example, a person’s ability to type a
sentence on a smartphone can be measured by both
counting typing errors and by measuring how the user
strikes keys using accelerometer and touchscreen data.
In this paper, we describe and evaluate five different drunk
user interfaces. We combine different drunk user interfaces
into a single smartphone app that creates a detailed
snapshot of a person’s abilities. We call this app the Drunk
User Interfaces app, or DUI (pronounced “doo-eee”).
What would motivate a person to use DUI in the first place?
We envision a number of possible use cases:
1. Services like OnStar from General Motors can
allow individuals to unlock their vehicles with
their smartphones
1
. A car insurance company
could offer a discount to customers who agree to
use DUI whenever they try to unlock their car after
10 PM or leave an establishment that serves
alcohol. If they fail DUI, their car will not start.
2. Bartenders are obliged to refuse service to
customers who seem overly intoxicated. Either a
bartender or a customer may wish to check their
1
https://www.onstar.com/us/en/services/services.html
Permission to make digital or hard copies of all or part of this work for
personal or classroom use is granted without fee provided that copies are
not made or distributed for profit or commercial advantage and that copies
bear this notice and the full citation on the first page. Copyrights for
components of this work owned by others than ACM must be honored.
Abstracting with credit is permitted. To copy otherwise, or republish, to
post on servers or to redistribute to lists, requires prior specific permission
and/or a fee. Request permissions from Pe[email protected].
CHI 2018, April 21–26, 2018, Montreal, QC, Canada
© 2018 Association for Computing Machinery.
ACM ISBN 978-1-4503-5620-6/18/04…$15.00
https://doi.org/10.1145/3173574.3173808

blood alcohol level (BAL) to ensure safe drinking
behavior.
3. Many teenagers fear “drunk texting” – when a
person sends a text message that they normally
would not because alcohol has impaired their
judgment. DUI failures could lock a person out of
his or her messaging app until the next day.
4. Individuals might benefit from increased self-
awareness or education about how they respond to
alcohol and how quickly their motor coordination
and cognition degrade.
DUI measures the side effects that alcohol has on a person’s
own abilities, not the alcohol concentration in a person’s
blood directly. Furthermore, some of our proposed use
cases only require a binary decision between sobriety and
inebriation, not a precise estimate of BAL. Nevertheless,
we strive to achieve the most difficult goal possible:
estimating a person’s BAL. We do this through a data-
driven approach. We collected data from 14 participants in
a 5-day longitudinal study where participants used DUI at
various BALs. This study design provides several benefits
over previous alcohol studies in the HCI community
[2,22,26], the main benefits being that it allows us to
account for learning effects and control for fatigue, which
can result in behavior that appears similar to inebriation.
Using a combination of five different drunk user interfaces,
DUI is able to estimate BAL with a mean absolute error of
0.005% ± 0.007% when the app accounts for the user’s
learning curve
2
.
The task interfaces comprising the design of DUI are not
necessarily novel; most of the tasks are borrowed from
literature in the HCI and medical communities [18,21,27].
Rather, their combination in DUI and their ability to
produce data that informs an accurate BAL estimate and
inebriation decision are the key breakthroughs in this paper.
The two primary contributions of this work are: (1) the DUI
app, comprising (a) tasks that challenge a person’s
psychomotor control in a mobile setting, and (b) the use of
machine learning to translate a person’s performance into a
BAL estimate; and (2) a 14-person longitudinal study of
DUI demonstrating its ability to track different BALs for
the same user against a breathalyzer baseline.
RELATED WORK
DUI draws inspiration from work at the intersection of
situational impairments and mobile devices. We briefly
highlight some of this work, followed by a summary of
research and products aimed at measuring BAL.
Situational Impairments
We view inebriation as a situational impairment
[36,40,41,46,51], i.e., a factor that affects a person’s ability
2
In the United States, BAL is typically reported as the fraction of
a person’s blood that contains alcohol by volume. The units are
interchangeable with g/dl (0.10% = 0.10 g/dl).
to interact with others and the world around them.
Situational impairments can be imposed by the user’s
external environment (e.g., cold weather [12]), by internal
changes (e.g., medicine-induced motor-impairment [45]), or
by a combination thereof (e.g., divided attention [34]).
Smartphones bring situational impairments to the forefront
because they are used in a variety of different mobile
scenarios [24]; at the same time, smartphones are
instrumented with sensors that can interpret and understand
these scenarios, providing the opportunity for ameliorating
the effects of situational impairments within them [50].
These works and others view situational impairments as
problems that can be addressed by sensing the user’s
current state and adapting the interface accordingly. In this
work, however, we stop short of adapting the interface and
instead use the sensed indicators of the user’s state to train a
machine learning model that outputs a description of the
user’s state – specifically a BAL measurement.
Hardware for Measuring Alcohol Consumption
Breathalyzers are the de facto method of measuring BAL
outside of a medical setting [4]. Most people are familiar
with the handheld breathalyzers carried by law
enforcement, but companies have produced different form
factors for personal use. For example, Tokyoflash
3
produces an LCD watch with a built-in breathalyzer for
$139.00 USD. At one point, Breathometer
4
produced a
breathalyzer that could interface with a smartphone via the
audio jack or Bluetooth, for $49.99 and $99.99 USD,
respectively; the FTC later initiated an investigation and
found their accuracy claims to be false
[9].
There are other methods for measuring BAL that are meant
to be easier than a blood draw. TruTouch
5
is a device that
measures BAL non-invasively using a method called
photoplethysmography (PPG). Alcohol slightly changes the
blood’s color, which can be quantified by shining different
wavelengths of light onto the fingertip and measuring the
intensity that is reflected back. SCRAM has a device that
measures BAL through the wearer’s perspiration every 30
minutes
6
. The device is intended for high-risk drunk driving
offenders who are court-ordered to monitor their drinking
behavior. Finally, Jung et al. [25] developed a smartphone
attachment that performs color analysis on pads that react to
saliva.
Each of these systems is able to measure BAL at some
biological level; however, these systems either require the
purchase of extra hardware or certain specifications from a
person’s smartphone. We view these as limitations towards
3
https://www.tokyoflash.com/en/watches/kisai-intoxicated-
silicone
4
https://www.breathometer.com/
5
http://tttinc.com/
6
https://www.scramsystems.com/products/scram-continuous-
alcohol-monitoring/

ubiquitous BAL sensing, which is why we propose drunk
user interfaces that can work on an unmodified smartphone.
Mobile Software for Measuring Alcohol Consumption
Because smartphones are ubiquitous, researchers have
explored ways that mobile devices can be used to curb
alcohol abuse without supplemental hardware. One area
where smartphones have been used is education. Hundreds
of publicly available apps, such as BAC Calculator
7
and
IntelliDrink PRO
8
, allow users to log their drinking
behavior. Using demographic information (e.g., height,
weight) and data on the drinks themselves (e.g., proof,
frequency, quantity), these apps estimate the users’ BAL;
however, a study by Weaver et al. [47] found that the
estimates reported by 98 such apps were inaccurate
compared to a breathalyzer. Of course, these apps also rely
on self-report, which is prone to error.
Shifting to more automatic means of sensing inebriation,
Hossain et al. [22] mined geotagged tweets to determine
whether or not people were drunk. They assumed that
tweets with words like “hangover” and “drunk” came from
drunk individuals. They then propagated that inference to
tweets that were posted by the same person near that time.
One of the most common tasks explored by the HCI and
ubicomp communities for predicting inebriation is gait
analysis. The vision of these projects is an app that
continuously processes the smartphone’s accelerometer
data for features such as step amplitude and cadence
variation [2,26]. BreathalEyes [5] reports a BAL estimate
by detecting nystagmus, or involuntary eye movement,
during horizontal gaze shifts. To the best of our knowledge,
there is no publicly available study that describes
BreathalEyes’ accuracy. Our work is most similar to that of
Bae et al [3], who detected heavy drinking episodes in a
study involving the collection of mobile sensor data and
experience sampling methods for ground truth. Their sensor
data included location, network usage, and motion data.
Unlike our work, Bae et al. did not use human performance
data. They also made a categorical assessment (sober, tipsy,
or drunk), not a continuous-scale BAL estimate as we do.
THE DESIGN OF DUI
The DUI app comprises five different drunk user interfaces:
(1) typing, (2) swiping, (3) balancing+heart rate, (4) simple
reaction, and (5) choice reaction. For each task, we cite a
subset of clinical experiments that informed them, how they
were adapted for use on a mobile device, and some of the
features calculated on human performance and sensor data.
Unfortunately, limitations of space preclude a complete
listing of every feature used for each task. A more detailed
listing can be found on the project’s webpage
9
. We then
7
https://play.google.com/store/apps/details?id=com.simonm.blood
alcoholcontentcalculator
8
https://itunes.apple.com/us/app/intellidrink-pro-blood-alcohol-
content-bac-calculator/id440759306
9
https://atm15.github.io/extra/DUI_feature_list.csv
describe how those features are processed and analyzed to
produce a final BAL estimate.
(1) Typing Task
DUI’s typing task is intended to measure the user’s fine
motor coordination abilities and cognition as they text.
Anecdotal evidence suggests that texting is more difficult
while a person is inebriated; to the best of our knowledge,
though, there has been no work that has quantitatively
analyzed the effect of alcohol on smartphone touchscreen
typing. However, research in medicine and psychology has
examined similar tasks that require small, controlled
movements, such as the Purdue Pegboard Test [6].
For DUI’s typing task, the user is presented with a random
phrase from the MacKenzie-Soukoreff phrase set [33] and
asked to type the phrase “as quickly and accurately” as
possible, relying on their own internal speed-accuracy
tradeoff. Auto-correct is disabled, and no cursor is provided
for the user to jump back to make corrections; if the user
makes a mistake, they must decide for themselves whether
or not to remedy the mistake with a backspace or to leave it.
We imposed these restrictions in keeping with standard text
entry evaluation methodology [52].
There are two levels of features that emerge from this test.
At a high level, DUI utilizes the error rate analysis
proposed by Soukoreff and MacKenzie for text entry
analysis [42]. In such an analysis, each character is
classified into one of four categories: “correct” (C), “fix”
(F), “incorrect fixed” (IF), and “incorrect not fixed” (INF).
DUI calculates different text entry metrics involving these
character categories that not only measure how often the
user made mistakes, but also how often they decided to
correct those mistakes. Other quantities that can be
calculated include “utilized bandwidth” (i.e., the fraction of
correct keystrokes made) and “participant
conscientiousness” (i.e., the fraction of mistakes corrected):
At a lower level, DUI examines the mechanics of the user’s
typing through the touchscreen, accelerometer, and
gyroscope, similar to how Goel et al. [16] used those
sensors to compensate for typing errors that were made
while walking. DUI’s typing task uses a custom keyboard,
similar in appearance to the smartphone’s default keyboard,
which records the precise position and radius of each touch.
From this data, DUI calculates features like the Euclidean
distance between the center of the selected key and the
user’s touch position. Motion sensor features include the
peak acceleration before a touch and variation in phone
orientation during the task. One interesting hypothesis
within this task is that people could have different reactions
to mistakes that could be detected through sensor data. If a
person is drunk, they could overreact to the mistake and
jostle their hand in a more pronounced manner than if they
were sober; on the other hand, they may overlook the
mistake and not react at all.
(2) Swiping Task
Whereas the DUI typing task measures fine motor control
in the form of repeated target selection, the swiping task
measures fine motor control through gesturing. The swiping
task can be considered a progressive goal-crossing task
where the user is asked to pass through different targets [1].
For feature extraction, we also treat the swiping task as a
steering task with implicit tunnels. To our knowledge, the
effect of inebriation on swiping gestures has yet to be
explored, but there have been related studies involving
tracing. Hindmarch et al. [21], for example, saw that
participants’ ability to track a moving target with a joystick
worsened after consuming alcohol.
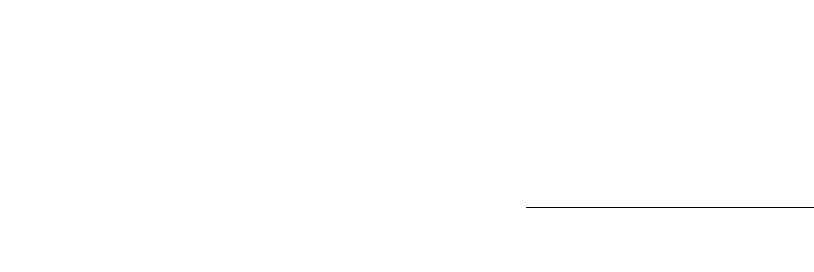
The swiping task shows a screen that mimics the 3×3 lock
screen of many Android devices (Figure 1). The user traces
a random 4-digit passcode on the screen. The passcode is
generated in such a way so that the user must change the
direction of his or her finger after each digit. Each circular
cell in the grid has a moderate diameter, but a digit is only
triggered if the user’s finger passes over the small gray
center.
Although the user believes that they are simply entering a
passcode for accuracy, the features DUI calculates for the
swiping task come from comparing the trajectory of the
user’s finger (solid trace, Figure 1) to the ideal 3-segment
shape that connects the 4 digits (dashed lines, Figure 1).
The user does not see the ideal trajectory, only their own
trace. Of course, the user is not expected to move their
finger from point-to-point in the most efficient manner
possible, but the hypothesis is that the user’s finger would
move more efficiently while sober than while drunk. One
metric we use to compare the gesture shapes is the
proportional shape matching metric described by
Kristensson and Zhai [30], which compares the form of two
shapes regardless of when their points are sampled. We also
examine each gesture segment individually by slicing the
data between the time when the user’s finger enters and
exits the gray center of the digit cell. For each segment, we
calculate the path-based accuracy features proposed by
MacKenzie et al. [32] for evaluating how a trajectory
between two points deviates from the shortest path between
them. For example, “movement variability” measures the
standard deviation of the distance between the ideal path
and the user’s trajectory. Finally, we also calculate time-
based measurements, such as maximum finger velocity,
acceleration, and jerk, for each segment; these features were
found to be informative by Flash and Hogan for
characterizing human motion [15].
(3) Balancing+Heart Rate Task
DUI’s balancing+heart rate task serves two purposes. The
original intent of the task was to measure just the user’s
heart rate; a person’s average heart rate slows down after
alcohol consumption because of alcohol’s depressive
effects [39]. Han et al. [18] recently demonstrated a method
of measuring heart rate using a technique called
photoplethysmography (PPG) through the smartphone
camera. In short, PPG measures the transparency of the
finger as blood rushes in and out while circulating. For the
PPG measurement to be clear, the user must hold his finger
completely still on the camera. We realized that this also
offers the chance for a test that challenges the user’s
coordination while their heart rate is being measured. For
example, Tianwu et al. [43] cite diminished vestibular
control with alcohol consumption.
In our DUI task, the user is instructed to hold the
smartphone parallel to the floor. The user is then told to
place their index finger over the flash and the camera
simultaneously so that their heart rate can be measured for
10 seconds. The user sees two widgets on the bottom of the
screen. One widget shows a preview of what the camera
sees so that the user can adjust his or her fingertip if it is not
in the correct position. The other widget shows a constantly
updated “flatness score” that the user is supposed to keep as
high as possible; unbeknownst to the user, the score is a
function of the accelerometer reading along the z-axis (i.e.,
through the screen).
The features for the balancing+heart rate task relate to both
the user’s heart rate and their ability to keep the smartphone
flat. The user’s average heart rate is measured using Han et
al.’s PPG algorithm [18] from the camera video. If the
calculation fails or the algorithm misses a couple of beats,
DUI uses that as an indication that the user was unable to
comply with the instructions, which could indicate
inebriation. The user’s ability to maintain balance with his
or her hand is measured using the standard deviation of the
acceleration in the z-direction.
(4) Simple Reaction Task
DUI’s simple reaction task is intended to capture the user’s
alertness and, to a lesser extent, motor speed. Multiple
Figure 1. The DUI swiping task resembles an Android 3×3 lock
screen. The straight dashed red lines show the ideal gesture
(hidden from the user) for the code 1-5-8-9, while the curvy
solid green path shows the user what they have drawn.
studies [21,37] have linked alcohol consumption to
impaired reaction times. DUI’s task for measuring reaction
is a variation of PVT-Touch [27], a smartphone-based
version of the clinically validated Psychomotor Vigilance
Task (PVT) by Dinges and Powell [11] to measure
alertness. DUI utilizes two of the four touchscreen input
techniques that were investigated in Kay et al.’s work on
PVT-Touch: “touch down” and “finger lift”. These gestures
were selected because Kay et al. found that the “touch
down” gesture was most comparable to the traditional PVT
and the “finger lift” gesture was the most precise.
For DUI’s simple reaction task, the user is asked to perform
a “touch down” gesture and then a “finger lift” gesture in
response to a randomly-timed stimulus. That stimulus is a
single square shown in the middle of the screen. When the
screen changes from red to green, the user must perform a
“touch down” gesture; when the square changes from green
to red, the user must perform a “finger lift” gesture. The
events were spaced within a 7-second period such that the
“touch down” would occur randomly within the first 3
seconds and the “finger lift” would occur randomly within
the last 3 seconds. The user was not instructed to use a
particular finger, but we found that most used their thumb.
From a human performance standpoint, DUI records the
time difference between the square’s color change and the
expected action, i.e., “touch down” or “finger lift”. From a
sensing standpoint, DUI records data from the touchscreen,
accelerometer, and gyroscope. It also records touch
pressure through the touchscreen and the motion of the
smartphone as the user performs the task.
(5) Choice Reaction Task
Like the simple reaction task, the choice reaction task is
intended to assess alertness and motor speed; we treat the
two tasks independently, as psychology has done. Instead of
the single square in the middle of the touchscreen, the
choice reaction task for DUI shows four squares arranged in
a 2×2 grid. Only one of the four squares, selected at
random, changes from red-to-green and then green-to-red.
In addition to the features described for the simple reaction
task, DUI also computes the user’s accuracy at selecting the
correct square.
Excluded Tasks
Many other tasks could be made into drunk user interfaces,
each with their own intended purpose, benefits, and
drawbacks. We explored a few in concept or in practice.
For example, we considered walking [2,26], but felt that
requiring the user to move would lead to a poor user
experience. We also considered speech analysis [7,28], but
the diversity of accents led to difficulties. Finally, we
considered short term memory [38], but the typical word
recall task simply took too long (over one minute).
Machine Learning
Each task generates a set of human performance metrics
that can be used as features for training a regression model
that estimates BAL. Not only are the human performance
metrics of an individual trial interesting, but also the
variation of those metrics across different trials. For
instance, a person may have the same average reaction time
when they are sober and when they are drunk, but they may
have a larger spread of times while drunk. In our user study,
we asked participants to perform each task multiple times.
The performance metrics across different trials of the same
task are aggregated using means and standard deviations.
Fifty-one features are available for training, but some are
more informative for estimating BAL than others.
Automatic feature selection is used to select the most
explanatory features and eliminate redundant ones. The top
25% of the features that explain the data according to the
mutual information scoring function are used in the final
models. Mutual information measures the dependency
between two random variables [29]. Automatic feature
selection works best when all of the features are normally-
distributed. We assume that this is the case with most of the
features except for those that are time-based (e.g., reaction
times). Prior research has noted that such measures tend to
be log-normally distributed [8,31], so they are log-
transformed after they are aggregated before feature
selection and training.
DUI uses random forest regression models [44] for
estimating BAL. A single decision tree regressor would
force features to be split sequentially in the same tree;
random forest regression learns shallower, more isolated
trees instead, reducing the possibility of nonsensical
interactions between features across tasks. The
disadvantage of random forest regression is that it cannot
extrapolate beyond the BAL levels that were reached in the
study. Models like linear regression can extrapolate,
although there is no guarantee that they would do so
correctly. We chose random forest regression because it
outperformed the other models we tried for the data we had.
The feature extraction and machine learning models were
built in Python using the scikit-learn package.
USER STUDY FOR DUI
We conducted a longitudinal user study of DUI with the
intent of collecting human performance data at different
BALs for the same users over time. Our study design
allowed us to control for fatigue while modeling any
learning that occurred as users gained familiarity with
DUI’s tasks.
Participants
Fourteen participants (9 male, 5 female) ranging from 21 to
35 years old (M = 25.7, SD = 4.8) were recruited for our
study. The participants were a mix of Caucasian, Asian, and
South Asian races. All participants owned and used a
smartphone on a daily basis.
Apparatus
Participants used our custom smartphone app on a third-
generation Moto G smartphone that has a 5-inch capacitive

screen with 720×1080 pixels. The app was designed with
five different screens, one for each of the drunk user
interfaces. Each time a person used DUI, they saw the
typing, swiping, and balancing+heart rate task in that order
five times; after that, they saw the simple reaction task five
times in a row, and then the choice reaction task five times
in a row. In other words, one “use” of DUI entailed five
trials of each task in our study. The task order was selected
for the participants’ convenience.
Each screen had a consistent presentation, including
instructions at the top, a button to start and stop the task,
and a red “recording light” icon to indicate when data was
being recorded. Navigation between the tasks happened
automatically; even if the participant felt that they made a
mistake, redoing tasks was disallowed and the app
progressed to the next screen.
Procedure
Prospective participants were required to satisfy guidelines
set by the National Advisory Council on Alcohol Abuse
and Alcoholism (NIAAA)
10
in order to participate in the
study. They also had to provide state- or federally-approved
identification that verified that they were at least 21 years
old, the legal drinking age in the United States. Participants
also had to confirm that they did not have a family history
of alcoholism and that they were not taking any medication
that interacted with alcohol. Finally, in accordance with the
NIAAA and at the insistence of our IRB, female
participants were required to take a pregnancy test on the
first day of the study to confirm that they were not
pregnant.
Participants satisfying those criteria were scheduled to
participate in our study for five sessions. The sessions were
scheduled in 24-hour intervals with a tolerance of one hour;
if there was a scheduling conflict, the remaining sessions
were pushed by another 24 hours to maintain time-of-day.
No two sessions were scheduled more than 48 hours apart.
Maintaining this schedule was important as it allowed us to
control for time-of-day related fatigue. Had participants
done one session in the afternoon and another session late at
night, the latter session would have included the
confounding effects of fatigue. The default schedule was
each weekday (Monday through Friday) at 4 PM. Although
4 PM is earlier than when most people start drinking,
starting early helped make each session quicker since it was
right before people had eaten dinner.
In the first session, the participant was introduced to DUI.
A research staff member explained each task, but did not
mention the specific metrics that were being recorded.
Participants were allowed to operate the smartphone with
their own texting style (e.g., one finger, two thumbs, etc.)
and swiping posture. The only restriction was that they had
to hold their phone in their hands.
10
http://www.niaaa.nih.gov/Resources/ResearchResources/job22.
htm
Once the participant had used DUI in the first session, they
were free to leave. The remaining four sessions started with
the participant using DUI sober as before. Once the
participant finished using DUI sober, he or she was required
to reach a predetermined BAL between 0.02% and 0.08%
in increments of 0.02%. The alcohol levels were increased
incrementally for all participants as a safety precaution; if
someone felt uncomfortable at a lower BAL, they were free
to withdraw without consequence.
The decision to use 0.08% as the maximum BAL was for
both safety and practicality. The NIAAA recommends that
research participants not be given more alcohol than they
would normally consume unless absolutely necessary; we
decided with our IRB that 0.08%, the legal limit in the
United States, would be a reasonable limit. Another
relevant guideline was that participants should not leave the
study until they were back below 0.04% to ensure they
would not drive while impaired. Increasing the upper BAL
limit would have led to a longer study and possibly more
attrition.
To reach the target BAL, we used the same procedure as
Hashtroudi et al. [20]. The research staff member estimated
the amount of alcohol needed based on the participants’
weight, the prescribed frequency of alcohol administration,
and the alcohol’s proof
11
. Based on that estimate, the
participant was given one shot of 80-proof vodka (1.5 fluid
ounces, 40% alcohol) every ten minutes. Once the alcohol
was consumed, participants waited for 15-20 minutes to
allow their bodies to absorb the alcohol. Participants then
had their BAL measured with a breathalyzer after rinsing
their mouths with water. Participants used DUI once their
BAL was within 0.003% of the target. If their BAL was too
low, they were given at most one shot and then delayed for
their body to absorb the alcohol; if their BAL was too high,
they waited and periodically used the breathalyzer until
they reached the target. If a participant’s BAL did not reach
the target within two hours, he or she used DUI at their
current BAL regardless.
Participants took 261.1 ± 27.4 seconds on average to use
DUI once in its entirety, including five trials of the five
tasks. The only two tasks that did not have a fixed duration
by design were the typing (10.8 ± 6.7 s) and swiping (3.4 ±
2.2 s) tasks.
Design & Analysis
Early on, we found that a model without any user-specific
adjustments would be infeasible. Each participant had their
own baseline abilities, which made it difficult to compare
results across users. Two different methods of user-specific
calibration were explored to account for this confound.
The first method compares performance to that of the sober
first session (Figure 2, left). This would be akin to asking
11
http://www.clevelandclinic.org/health/interactive/alcohol_calcul
ator.asp

the user to go through DUI once upon installation. Rather
than using the raw performance metrics calculated from a
particular session, the features given to the model are the
difference between a given session’s features and those
from the initial session. The problem with this approach is
that it does not account for learning.
The second method compares performance to a learning
curve fit to sober measurements taken at the beginning of
each session (Figure 2, right). The measures recorded when
the participant was sober were collected and indexed
according to the number of times the participant had used
DUI before (i.e., 0
th
, 1
st
, 3
rd
, 5
th
, and 7
th
). The metrics were
then individually fit to exponential learning curves of the
following form:
where is the session number index, Y is the performance
measure, and and are regression coefficients for the
user’s baseline and learning rate, respectively. Once this
learning curve was found, the contribution due to alcohol
consumption could be isolated by subtracting the
contribution of learning estimated for that given session.
Not all metrics were considered learnable. Features that
were considered performance-based (e.g., swiping
accuracy, reaction time) were fit to learning curves,
whereas more biological-based features (e.g., heart rate,
typing motion acceleration) were not.
All experiments were conducted using leave-one-out cross-
validation across users. In other words, to generate results
for DUI for each participant, that participant’s data was
excluded from training DUI’s models. Once the models
were trained, three different measures were obtained: (1)
the absolute mean error of DUI’s BAL estimates compared
to the breathalyzer readings, (2) the Pearson correlation
coefficient of DUI’s BAL estimates compared to the
breathalyzer readings, and (3) sensitivity (true positive) and
specificity (true negative) rates when classifying individuals
as sober or drunk. For our purposes, we set our model’s
decision boundary for sobriety at 0.04% in accordance with
the National Advisory Council on Alcohol Abuse and
Alcoholism. In this context, sensitivity was defined as how
often DUI correctly identified drunk individuals, whereas
specificity was defined as how often DUI correctly
identified sober individuals.
RESULTS
In this section, we present the results of three different
experiments. The first experiment determined whether DUI
would perform better with a single calibration session or
multiple. The second experiment investigated whether or
not multiple trials for the same drunk user interface had an
effect on performance. The third experiment examined how
well DUI can estimate BAL when multiple drunk user
interfaces are combined.
It should be noted that two participants did not complete the
entire protocol. One participant withdrew after the third
session because she was uncomfortable reaching an
elevated BAL, while the other withdrew after the fourth
session because of short-notice travel plans. Nevertheless,
their data is included in our analysis since they went
through enough of the protocol to experience different
BALs. This means that (12 participants × 5 sessions) + (1
participant × 4 sessions) + (1 participant × 3 sessions) = 67
sessions were included in our analyses.
Methods of User-Specific Calibration
Our first experiment compared the two methods of user-
specific calibration: single-day baseline and learning curve
Figure 2. Idealized illustrations of two user-specific calibration methods enabled by the study design: (left) single-day baseline,
where all performance metrics are compared to the first session, (right) learning curve, where all performance metrics are compared
to a learning curve fit to the sober data. Our evaluation reveals that calibration with a learning curve leads to better accuracy results.

(Figure 2). All tasks and all trials were used for this analysis
to provide the most information possible to the regression
models. Using the single-day baseline, DUI achieved an
absolute mean error of 0.015% ± 0.013%, much higher than
the breathalyzer’s claimed accuracy of 0.005%. DUI with
the single-day baseline also had a Pearson correlation
coefficient of 0.73. The model generally underestimated
user BAL by an average of 0.002%; however, the model led
to a sensitivity of 81.8% and a specificity of 61.8%. The
absolute mean error of the model that factored in learning
across multiple sessions was 0.005% ± 0.007, and the
Pearson correlation coefficient was 0.96. Unsurprisingly,
both the sensitivity (87.9%) and specificity (91.2%) of that
model were better than the model calibrated off the single
sober session. Although less practical, accounting for user
learning led to much stronger results. Participants clearly
became familiar with DUI, showing that the single
calibration session was insufficient. The results for the
other experiments calibrate using multiple sessions.
Single Task
The second experiment investigated the efficacy of each
task individually for predicting BAL. Table I shows the
absolute mean error and Pearson correlation coefficients for
the regression models trained using a different number of
trials of the same task. As a reminder, study participants
performed five trials of each task whenever they used DUI.
All possible combinations of trials were used for training
and testing to ensure that the random selection of an outlier
would not skew the results. Doing so yielded more training
and testing samples when two or three trials are used since
. More training samples can improve
accuracy by providing the model with more examples,
while more testing samples can worsen accuracy by
challenging the model with more outliers. Keeping the
same number of samples would have subjected the results
to random selection.
Table II lists the features that were selected through
automatic feature selection; the descriptions of these
features can be found at the project’s webpage
9
. Note that
the features selected from this experiment were not
necessarily the ones that were selected when tasks were
combined since feature selection depends on features that
complement one another.
Using more trials did not have a significant effect on the
results. Although more trials would be expected to better
represent the user’s performance, using multiple
combinations of fewer trials compensated for that effect.
The choice reaction task performed well on its own,
yielding Pearson correlation coefficients greater than 0.90;
the other tasks did not exceed 0.75.
Multiple Tasks
Our final experiment examined how combining features
across tasks could improve DUI’s results. Table III shows
the absolute mean error and Pearson correlation coefficients
for all possible combination of tasks. For this analysis, all
five trials of each task were included.
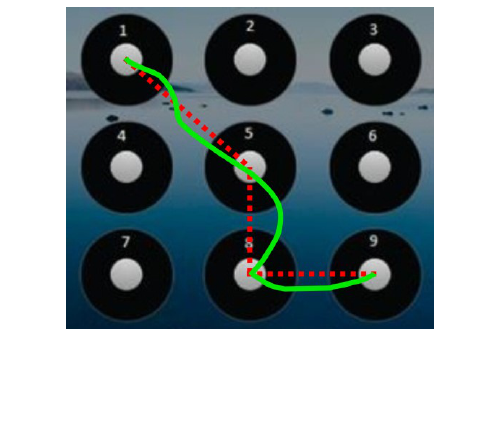
Table I. Absolute mean error and Pearson correlation coefficient using different numbers of trials for the same task.
1 trial
2 trials
3 trials
4 trials
5 trials
Task
Error
(%)
r
Error
(%)
r
Error
(%)
r
Error
(%)
r
Error
(%)
r
T
0.017 ±
0.016
0.65
0.017 ±
0.016
0.64
0.019 ±
0.018
0.55
0.018 ±
0.018
0.58
0.016 ±
0.015
0.68
S
0.017 ±
0.015
0.65
0.016 ±
0.015
0.66
0.016 ±
0.013
0.72
0.016 ±
0.015
0.67
0.015 ±
0.015
0.69
BHR
0.019 ±
0.019
0.54
0.020 ±
0.018
0.53
0.019 ±
0.019
0.55
0.020 ±
0.019
0.53
0.017 ±
0.018
0.57
SR
0.017 ±
0.017
0.63
0.018 ±
0.017
0.60
0.018 ±
0.017
0.60
0.018 ±
0.017
0.59
0.017 ±
0.016
0.65
CR
0.004 ±
0.009
0.95
0.004 ±
0.007
0.96
0.005 ±
0.008
0.94
0.004 ±
0.007
0.96
0.001 ±
0.008
0.97
T = typing, S = swiping, BHR = balancing+heart rate, SR = simple reaction, CR = choice reaction
Table II. Selected features for the single task experiment.
Task
Most important features
Typing
Mean touch radius while lifting
Mean distance from key center
Mean force during touch
Mean touch duration
Swiping
Mean segment speed
Min segment speed
Min segment jerk
Mean throughput
Mean touch radius
Balancing+
Heart Rate
Mean heart rate
Simple
Reaction
Mean finger lift time
Choice
Reaction
Mean finger lift time
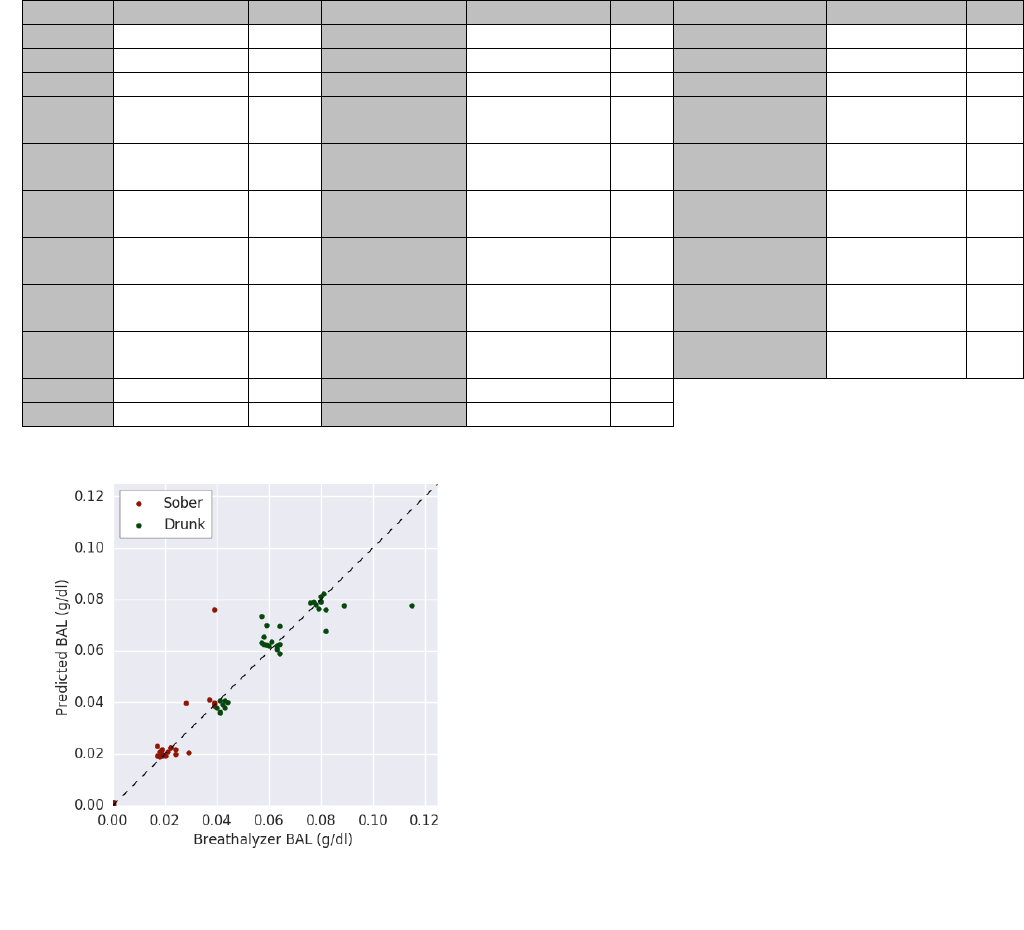
Although many combinations of tasks lead to similar
performance results as the individual tasks, we found some
combinations to be more promising. Using all of the tasks
together led to an absolute mean error of 0.005% ± 0.007%
and a Pearson correlation coefficient of 0.96 (Figure 3). The
estimates have a slightly positive bias, overestimating by an
average of 0.0005% across all BALs. Not all tasks were
needed, though, as we found through the previous
experiments that the choice reaction task performed well on
its own. Combining that task with the typing or swiping
tasks added to DUI’s complexity without compromising
accuracy, which is important if a user becomes practiced at
the choice reaction task on its own.
To frame the results in a different manner, DUI can be
treated as a classifier that determines whether or not a
person should operate a vehicle. The National Advisory
Council on Alcohol Abuse and Alcoholism defines a person
to be sober at or below 0.04% BAL. With that decision
threshold and using all of the tasks, DUI leads to a
sensitivity of 93.9% and a specificity of 82.3%. Like any
other model with a decision boundary, DUI’s threshold can
be tuned for a specific need; the threshold can be decreased
to increase specificity at the cost of lower sensitivity, or the
reverse could be done. As a point of comparison for the
results, Bae et al [3] reported 96.6% accuracy when
separating between three categories of inebriation. That
being said, their results are not necessarily comparable
since they were drawn from self-reports on the number of
drinks consumed.
DISCUSSION & LIMITATIONS
Our goal was to develop a smartphone app that assesses a
person’s psychomotor control and translates that assessment
into an estimate of their BAL without the need for
additional hardware. To achieve this, we developed and
evaluated DUI, a combination of five different tasks that
challenge a person’s motor coordination and cognition. DUI
uses random forest regression to combine human
performance metrics and features derived from smartphone
sensor data to estimate a person’s BAL. We conducted a
week-long study to train and evaluate DUI. Through this
study, we found that by accounting for user learning
through multiple sessions (Figure 2, right), DUI is able to
estimate BAL with a mean absolute error of 0.005% ±
0.007% relative to a breathalyzer. This means that in order
for people to use the DUI, they would have to perform the
tasks periodically while sober. DUI will likely not work if a
user purposefully botches a baseline. For scenarios when
Table III. Absolute mean error and Pearson correlation coefficient using different tasks.
Test
Error (%)
r
Test
Error (%)
r
Test
Error (%)
r
T
0.016 ± 0.015
0.68
S+CR
0.005 ± 0.007
0.96
S+ BHR+CR
0.005 ± 0.007
0.96
S
0.015 ± 0.015
0.69
BHR+SR
0.017 ± 0.017
0.58
S+SR+CR
0.005 ± 0.007
0.96
BHR
0.017 ± 0.018
0.57
BHR+CR
0.016 ± 0.014
0.69
BHR+SR+CR
0.015 ± 0.014
0.69
SR
0.017 ± 0.016
0.65
SR+CR
0.016 ± 0.015
0.68
T+S+
BHR+SR
0.015 ± 0.014
0.71
CR
0.001 ± 0.008
0.97
T+S+BHR
0.014 ± 0.013
0.76
T+S+
BHR+CR
0.004 ± 0.007
0.96
T+S
0.014 ± 0.013
0.75
T+S+SR
0.014 ± 0.013
0.76
T+S+
SR+CR
0.005 ± 0.007
0.96
T+BHR
0.014 ± 0.014
0.74
T+S+CR
0.014 ± 0.013
0.75
T+BHR+
SR+CR
0.013 ± 0.012
0.78
T+SR
0.014 ± 0.014
0.73
T+BHR+SR
0.014 ± 0.014
0.74
S+BHR+
SR+CR
0.004 ± 0.007
0.96
T+CR
0.005 ± 0.007
0.96
T+ BHR +CR
0.014 ± 0.014
0.74
T+S+BHR+
SR+CR
0.005 ± 0.007
0.96
S+BHR
0.015 ± 0.014
0.71
T+SR+CR
0.014 ± 0.014
0.73
S+SR
0.014 ± 0.014
0.74
S+BHR+SR
0.014 ± 0.015
0.72
T = typing, S = swiping, BHR = balancing+heart rate, SR = simple reaction, CR = choice reaction
Figure 3. The correlation plot showing DUI’s BAL predictions
with all 5 trials of all 5 tasks against the breathalyzer output.

DUI is used for enforcement (e.g., the car insurance
scenario), baselines can be recorded under the supervision
of a trusted entity (e.g., an insurance agent). Future studies
could be conducted to examine the differences between
how drunk people and non-compliant users fail tests,
perhaps differently.
Some clinical studies incorporate a placebo into their
protocol to ensure that participants are not simply acting
drunk after being given alcohol [48]. Our protocol did not
have a placebo condition because we did not have enough
participants to utilize some in a purely placebo condition.
There are two undesirable scenarios from a human
performance perspective. The first is when a person is given
alcohol but tries to act sober when using DUI. Participants
were instructed to complete each task to the best of their
abilities to avoid these issues. On the other hand, a
participant could be given a placebo but act intoxicated.
Although this scenario is not included in our dataset, the
cost of a false positive from DUI is much less than that of a
false negative (i.e., mild inconvenience vs. serious danger).
A limitation of DUI is that it does not measure BAL
directly, but rather the behavioral manifestations of
inebriation. Many researchers have noted similar symptoms
between inebriation and sleepiness, including impairments
to hand-eye coordination and short-term memory [10,49].
In fact, the source of inspiration for DUI’s simple reaction
and choice reaction tasks, PVT-Touch [27], was designed
for sleep loss assessment. We designed our study such that
each session was held at roughly the same time of day to
reduce fatigue variance across sessions. With even more
participant cooperation, our study could be extended to
having multiple sessions each day (i.e., every morning,
afternoon, and evening for a week). Nevertheless, there are
many tasks that both sleep-deprived individuals and
inebriated individuals should not perform, so while
distinguishing between the two is technically interesting,
we believe that it is not crucial for many use cases.
Many would-be participants were eager to join our study,
but one or more of the study’s high demands (e.g., repeated
alcohol consumption, scheduling impositions, and
requirement of pregnancy testing) led them not to
participate. Unsurprisingly, younger people were far more
willing to overlook such burdens for the sake of research.
One way to shorten the protocol to a single day would be to
replace the breathalyzer ground truth with a clinical one
wherein participants’ BALs are manipulated through
intravenous infusion [17]. Changing BAL intravenously has
the additional benefit of higher accuracy and control,
although breathalyzers have been used in past clinical
alcohol studies [26,49]. Eventually, we decided against this
method for fear that participants would not operate the
smartphone naturally while in a clinical setting.
FUTURE WORK
We recognize that there is more work to be done to
demonstrate the generalizability of DUI and its constituent
drunk user interfaces. By conducting our study in a quiet
office space with seating, participants were not exposed to
additional situational impairments that would occur
outdoors or in a noisy bar. Doing the study itself in-the-wild
would have been difficult for repeated recruitment and
control over alcohol consumption; nevertheless, more work
needs to be done to investigate how DUI would perform in
such scenarios.
DUI, in its current instantiation, is an app that must be
explicitly operated by the user to produce an estimate.
There were many reasons for this, including control over
the stimuli that the participant saw and being able to record
fine-grained sensor data from a custom keyboard.
Nevertheless, we believe that all of the tasks that we have
selected map well to actions that users normally perform on
their smartphones. Many people use a swipe password to
unlock their smartphone, which was the inspiration for the
DUI swiping task. Texting is also a common action
performed for a variety of tasks, and prior work has shown
how text entry accuracy measures can be obtained from text
entry “in the wild” [13]. We believe it would be possible to
integrate DUI more fully into a user’s everyday smartphone
use. Another way that DUI could be consolidated is by
combining tasks in a game. For example, a game like Fruit
Ninja
12
entails swiping in response to random stimuli,
combining both the swiping and reaction tasks.
CONCLUSION
Incidents involving inebriation often occur because they
happen before an intervention can take place, highlighting
the need for a blood alcohol level (BAL) system more
ubiquitous than a breathalyzer. We have introduced drunk
user interfaces (DUIs), smartphone tasks that use sensing
and human performance metrics to estimate a person’s
BAL. The combination of different DUIs led us to create
the DUI app, which utilizes machine learning on human
performance and sensor data features to attain a more
complete snapshot of the user’s current state. To evaluate
DUI, we conducted a rigorous longitudinal study in which
participants used the app at different ground-truth BALs.
We trained models that accounted for learning and found
that DUI was able to estimate BAL with an absolute mean
error of 0.005% ± 0.007%. It is our hope that other
researchers will recreate our study or improve upon it with
their own tasks so that ubiquitous inebriation assessment
might become a reality.
ACKNOWLEDGMENTS
This work was supported by the National Science
Foundation under grant IIS-1217627, a Google Faculty
Award, and the Mani Charitable Foundation. We also thank
Abdullah Ali for his help with the study, as well as the
participants for their time.
REFERENCES
1. Johnny Accot and Shumin Zhai. 1997. Beyond
12
https://fruitninja.com/
Fitts’ law: Models for trajectory-based HCI tasks.
In Proceedings of the ACM Conference on Human
Factors in Computing Systems (CHI ’97), 295–302.
https://doi.org/10.1145/258549.258760
2. Zachary Arnold, Danielle LaRose, and Emmanuel
Agu. 2015. Smartphone Inference of Alcohol
Consumption Levels from Gait. In Proceedings -
2015 IEEE International Conference on Healthcare
Informatics, ICHI 2015, 417–426.
https://doi.org/10.1109/ICHI.2015.59
3. Sangwon Bae, Denzil Ferreira, Brian Suffoletto,
Juan C Puyana, Ryan Kurtz, Tammy Chung, and
Anind K Dey. 2017. Detecting Drinking Episodes
in Young Adults Using Smartphone-based Sensors.
Proceedings of the ACM on Interactive, Mobile,
Wearable and Ubiquitous Technologies 1, 2: 1–36.
https://doi.org/10.1145/3090051
4. Robert F Borkenstein and H W Smith. 1961. The
breathalyzer and its application. Medicine, Science
and the Law 1: 13. Retrieved March 23, 2017 from
http://msl.sagepub.com/content/2/1/13.short
5. Clay Bradley and Gage A Brasher. 2013.
Nystagmus evaluation system. Retrieved July 13,
2017 from
https://www.google.com/patents/US9042615
6. Robert L Breckenridge and R Scott Berger. 1990.
Locus of Control and Perceived Alcohol Ingestion
in Performance of a Fine Motor Skill.
Psychological Reports 66, 1: 179–185.
https://doi.org/10.2466/pr0.1990.66.1.179
7. Malcolm Brenner and JR Cash. 1991. Speech
analysis as an index of alcohol intoxication--the
Exxon Valdez accident. Aviation, space, and
environmental medicine 62, 9 Pt 1: 893–8.
Retrieved August 19, 2017 from
http://www.ncbi.nlm.nih.gov/pubmed/1930083
8. Stuart K Card, Thomas P Moran, and Allen Newell.
1983. The Psychology of Human-Computer
Interaction. L. Erlbaum Associates.
https://doi.org/10.1007/s13398-014-0173-7.2
9. Federal Trade Commission. 2017. FTC v.
Breathometer, Inc. 1–20. Retrieved from
www.ftc.gov/system/files/documents/cases/170123
breathometer_dkt._4-1_-_stipulated_order.pdf
10. Drew Dawson and Kathryn Reid. 1997. Fatigue,
alcohol and performance impairment. Nature 388,
6639: 235–235. https://doi.org/10.1038/40775
11. David F Dinges and John W Powell. 1985.
Microcomputer analyses of performance on a
portable, simple visual RT task during sustained
operations. Behavior Research Methods,
Instruments, & Computers 17, 6: 652–655.
https://doi.org/10.3758/BF03200977
12. Edward Elton, D Dumolo, and Colette A Nicolle.
2010. Have I just pressed something? The effects of
everyday cold temperatures on dexterity. IN:
Designing Inclusive Interactions: Inclusive
Interactions between. In 5th Cambridge Workshop
on Universal Access and Assistive Technology, 22–
25. Retrieved July 14, 2017 from
http://www.academia.edu/download/42191250/PU
B_20571_20The_20effects_20of_20everyday_20co
ld_20temperatures_20on_20dexterity.pdf
13. Abigail Evans and Jacob Wobbrock. 2012. Taming
Wild Behavior: The Input Observer for Obtaining
Text Entry and Mouse Pointing Measures from
Everyday Computer Use. In Proceedings of the
SIGCHI Conference on Human Factors in
Computing Systems, 1947–1956.
https://doi.org/10.1145/2207676.2208338
14. Federal Bureau of Investigation. 2014. Crime in the
United States - 2014. Retrieved July 4, 2017 from
https://ucr.fbi.gov/crime-in-the-u.s/2014/crime-in-
the-u.s.-2014/tables/table-29
15. T Flash and N Hogan. 1985. The coordination of
arm movements: an experimentally confirmed
mathematical model. The Journal of neuroscience
5, 7: 1688–1703. https://doi.org/4020415
16. Mayank Goel, Leah Findlater, and Jacob
Wobbrock. 2012. WalkType: Using Accelerometer
Data to Accomodate Situational Impairments in
Mobile Touch Screen Text Entry. In Proceedings of
the 2012 ACM annual conference on Human
Factors in Computing Systems - CHI ’12, 2687–
2696. https://doi.org/10.1145/2207676.2208662
17. S A Grant, K Millar, and G N Kenny. 2000. Blood
alcohol concentration and psychomotor effects.
British journal of anaesthesia 85, 3: 401–406.
https://doi.org/10.1093/bja/85.3.396
18. Teng Han, Xiang Xiao, Lanfei Shi, John Canny,
and Jingtao Wang. 2015. Balancing Accuracy and
Fun: Designing Camera Based Mobile Games for
Implicit Heart Rate Monitoring. In Proceedings of
the ACM CHI’15 Conference on Human Factors in
Computing Systems, 847–856.
https://doi.org/10.1145/2702123.2702502
19. Rolla N Harger. 1948. Chemical Tests for
Intoxication as an Aid to Traffic and Industrial
Safety. Industrial Medicine and Surgery 17, 2: 52–
56. Retrieved July 4, 2017 from
https://www.cabdirect.org/cabdirect/abstract/19482
701549
20. Shahin Hashtroudi, Elizabeth S Parker, Lynn E
DeLisi, Richard J Wyatt, and Sharon A Mutter.
1984. Intact retention in acute alcohol amnesia.
Journal of Experimental Psychology: Learning,
Memory, and Cognition 10, 1: 156–163. Retrieved
July 6, 2017 from
http://psycnet.apa.org/journals/xlm/10/1/156/
21. I Hindmarch, J S Kerr, and N Sherwood. 1991. The
effects of alcohol and other drugs on psychomotor
performance and cognitive function. Alcohol and
alcoholism 26, 1: 71–79. Retrieved July 14, 2017
from
http://www.ncbi.nlm.nih.gov/pubmed/1854375
22. Nabil Hossain, Tianran Hu, Roghayeh Feizi, Ann
Marie White, Jiebo Luo, and Henry Kautz. 2016.
Inferring Fine-grained Details on User Activities
and Home Location from Social Media: Detecting
Drinking-While-Tweeting Patterns in Communities.
Retrieved July 11, 2017 from
http://arxiv.org/abs/1603.03181
23. Amy Jewett, Ruth A Shults, Tanima Banerjee, and
Gwen Bergen. 2015. Alcohol-impaired driving
among adults—United States, 2012. Morbidity and
Mortality Weekly Report (MMWR) 64, 30: 814–
817. Retrieved July 4, 2017 from
https://www.cdc.gov/Mmwr/preview/mmwrhtml/m
m6430a2.htm
24. Peter Johnson. 1998. Usability and Mobility;
Interactions on the move. In First workshop on
human computer interaction with mobile devices.
25. Youngkee Jung, Jinhee Kim, Olumide Awofeso,
Huisung Kim, Fred Regnier, and Euiwon Bae.
2015. Smartphone-based colorimetric analysis for
detection of saliva alcohol concentration. Applied
Optics 54, 31: 9183–9.
https://doi.org/10.1364/AO.54.009183
26. Hsin-Liu (Cindy) Kao, Bo-Jhang Ho, Allan C Lin,
and Hao-Hua Chu. 2012. Phone-based gait analysis
to detect alcohol usage. In Proceedings of the 2012
ACM Conference on Ubiquitous Computing -
UbiComp ’12, 661–662. Retrieved July 11, 2017
from http://dl.acm.org/citation.cfm?id=2370354
27. Matthew Kay, Kyle Rector, Sunny Consolvo, Ben
Greenstein, Jacob Wobbrock, Nathaniel Watson,
and Julie Kientz. 2013. PVT-Touch: Adapting a
Reaction Time Test for Touchscreen Devices. In
Proceedings of the ICTs for improving Patients
Rehabilitation Research Techniques, 248–251.
https://doi.org/10.4108/icst.pervasivehealth.2013.25
2078
28. F. Klingholz, R. Penning, and E. Liebhardt. 1988.
Recognition of low-level alcohol-intoxication from
speech signal. Journal of the Acoustical Society of
America 84, 3: 929–935.
https://doi.org/10.1121/1.396661
29. LF Kozachenko and NN Leonenko. 1987. Sample
estimate of the entropy of a random vector.
Problemy Peredachi Informatsii 23, 2: 9–16.
Retrieved March 28, 2017 from
http://www.mathnet.ru/eng/ppi797
30. Per-Ola Kristensson and Shumin Zhai. 2004.
SHARK
2
: A Large Vocabulary Shorthand Writing
System for Pen-Based Computers. Proceedings of
the 17th annual ACM symposium on User interface
software and technology - UIST ’04 6, 2: 43–52.
https://doi.org/10.1145/1029632.1029640
31. RJ Lawrence. 1988. The log-normal as event–time
distribution. Dekker, New York, New York, USA.
32. I Scott MacKenzie, Tatu Kauppinen, and Miika
Silfverberg. 2001. Accuracy measures for
evaluating computer pointing devices. In
Proceedings of the SIGCHI conference on Human
factors in computing systems - CHI ’01, 9–16.
https://doi.org/10.1145/365024.365028
33. I Scott MacKenzie and R William Soukoreff. 2003.
Phrase sets for evaluating text entry techniques. In
CHI ’03 extended abstracts on Human factors in
computing systems - CHI ’03, 754–755.
https://doi.org/10.1145/765891.765971
34. Alexander Mariakakis, Mayank Goel, Md Tanvir
Islam Aumi, Shwetak N Patel, and Jacob O
Wobbrock. 2015. SwitchBack: Using Focus and
Saccade Tracking to Guide Users’ Attention for
Mobile Task Resumption. In Proceedings of the
ACM CHI’15 Conference on Human Factors in
Computing Systems, 2953–2962.
https://doi.org/10.1145/2702123.2702539
35. National Highway Traffic Safety Association. 2015.
Traffic Safety Facts. 2014 Data.
https://doi.org/http://dx.doi.org/10.1016/j.annemerg
med.2013.12.004
36. Allen F Newell. 1995. Extra-ordinary human-
computer interaction. Cambridge University Press.
Retrieved September 12, 2017 from
http://dl.acm.org/citation.cfm?id=215600
37. Mary E Nicholson, MinQi Wang, Collins O
Airhihenbuwa, Beverly S Mahoney, and Dolores W
Maney. 1992. Predicting alcohol impairment:
Perceived intoxication versus BAC. Alcoholism:
Clinical and Experimental Research 16, 4: 747–
750. Retrieved July 6, 2017 from
http://onlinelibrary.wiley.com/doi/10.1111/j.1530-
0277.1992.tb00671.x/full
38. Suchismita Ray and Marsha E Bates. 2006. Acute
alcohol effects on repetition priming and word
recognition memory with equivalent memory cues.
Brain and Cognition 60, 2: 118–127.
https://doi.org/10.1016/j.bandc.2005.07.009
39. J M Ryan and L G Howes. 2002. Relations between
alcohol consumption, heart rate, and heart rate
variability in men. Heart (British Cardiac Society)
88, 6: 641–2. Retrieved July 18, 2017 from
http://www.ncbi.nlm.nih.gov/pubmed/12433903
40. Andrew Sears and Julie A. Jacko. 2008. Physical
disabilities and computing technologies: An
analysis of impairments. Lawrence Erlbaum
Associates, Hillsdale, New Jersey.
https://doi.org/10.1201/9781410615862
41. Andrew Sears, Min Lin, Julie Jacko, and Yan Xiao.
2003. When computers fade: Pervasive computing
and situationally-induced impairments and
disabilities. HCI International 2, 3: 1298–1302.
42. R William Soukoreff and I Scott MacKenzie. 2003.
Metrics for text entry research: an evaluation of
MSD and KSPC, and a new unified error metric. In
Proceedings of the conference on Human factors in
computing systems - CHI ’03, 113–120.
https://doi.org/10.1145/642611.642632
43. H Tianwu, Yoshinori Watanabe, M Asai, K
Shimizu, S Takada, and K Mizukoshi. 1995. Effects
of alcohol ingestion on vestibular function in
postural control. Acta Oto-Laryngologica 115,
S519: 127–131.
https://doi.org/10.3109/00016489509121886
44. Tin Kam Ho. 1995. Random decision forests.
Proceedings of 3rd International Conference on
Document Analysis and Recognition 1: 278–282.
https://doi.org/10.1109/ICDAR.1995.598994
45. Shari Trewin. 2002. An invisible keyguard. In
Proceedings of the fifth international ACM
conference on Assistive technologies, 143–149.
https://doi.org/10.1145/638249.638275
46. Gregg C Vanderheiden. 1997. Anywhere, anytime
(+anyone) access to the next-generation WWW.
Computer Networks and ISDN Systems 29, 8:
1439–1446. https://doi.org/10.1016/S0169-
7552(97)00067-6
47. Emma R Weaver, Danielle R Horyniak, Rebecca
Jenkinson, Paul Dietze, and Megan Sc Lim. 2013.
“Let’s get Wasted!” and Other Apps:
Characteristics, Acceptability, and Use of Alcohol-
Related Smartphone Applications. JMIR mHealth
and uHealth 1, 1: e9.
https://doi.org/10.2196/mhealth.2709
48. JM Weiler, JR Bloomfield, GG Woodworth, AR
Grant, TA Layton, TL Brown, DR McKenzie, TW
Baker, and GS Watson. 2000. Effect of
fexofenadine, diphenhydramine, and alcohol on
driving performance. Annals of Internal Medicine
132, 5: 354–363. Retrieved August 21, 2017 from
http://annals.org/aim/article/713291/effects-
fexofenadine-diphenhydramine-alcohol-driving-
performance-randomized-placebo-controlled-trial
49. A M Williamson. 2000. Moderate sleep deprivation
produces impairments in cognitive and motor
performance equivalent to legally prescribed levels
of alcohol intoxication. Occupational and
Environmental Medicine 57, 10: 649–655.
https://doi.org/10.1136/oem.57.10.649
50. Jacob O Wobbrock. 2006. The Future of Mobile
Device Research in HCI. In Proc. CHI ’06
Workshops, 131–134. Retrieved January 6, 2018
from
http://faculty.washington.edu/wobbrock/pubs/chi-
06.05.pdf
51. Jacob O Wobbrock, Krzysztof Z Gajos, Shaun K
Kane, and Gregg C Vanderheiden. Ability-Based
Design. Communications of the ACM.
52. Jacob O Wobbrock and Brad A Myers. 2006.
Analyzing the input stream for character- level
errors in unconstrained text entry evaluations. ACM
Transactions on Computer-Human Interaction 13,
4: 458–489.
https://doi.org/10.1145/1188816.1188819
